Written by Lennart Bongartz and Denys Surkov. Post 3 of 7 in the CMPEC3 series. Published in Military Medicine. Follow for Post 4: Materiel.
The Number That Anchors the Medical Plan
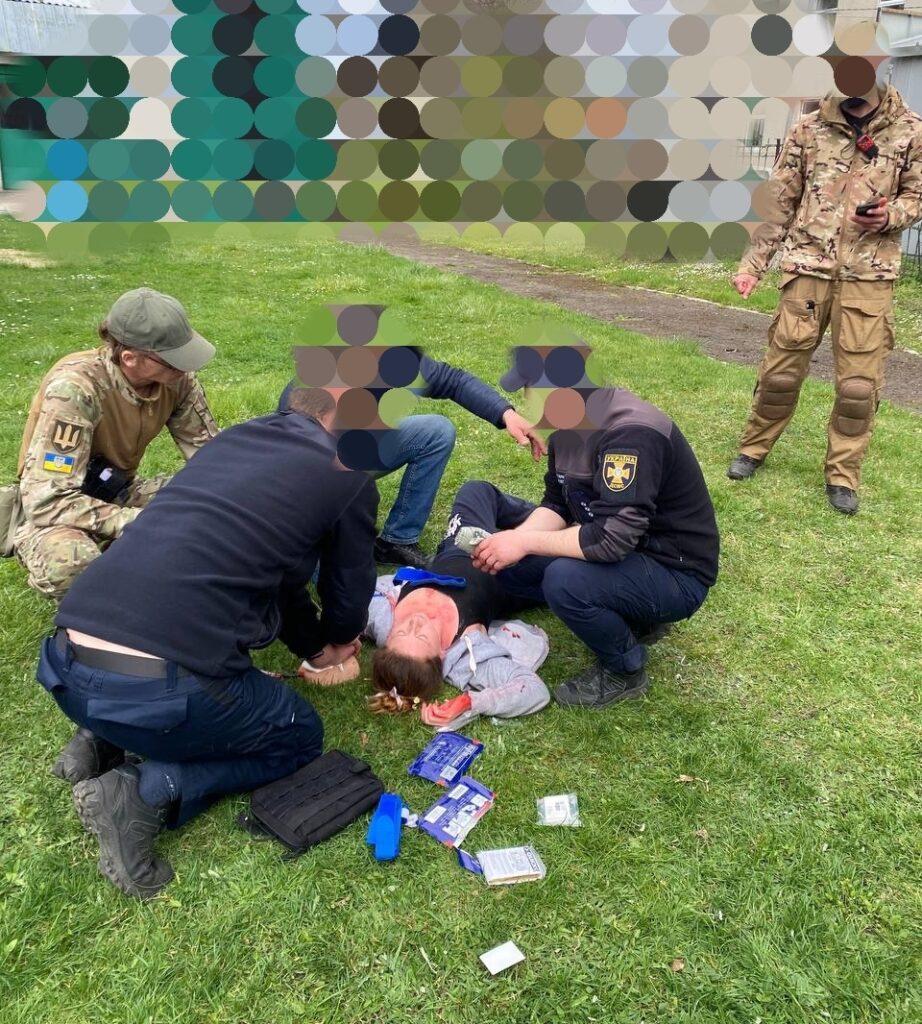
Before a single medical kit is packed or a CASEVAC route is plotted, the medical planner must answer the hardest question in battlefield medicine: how many casualties, of what type, arriving when, and from where?
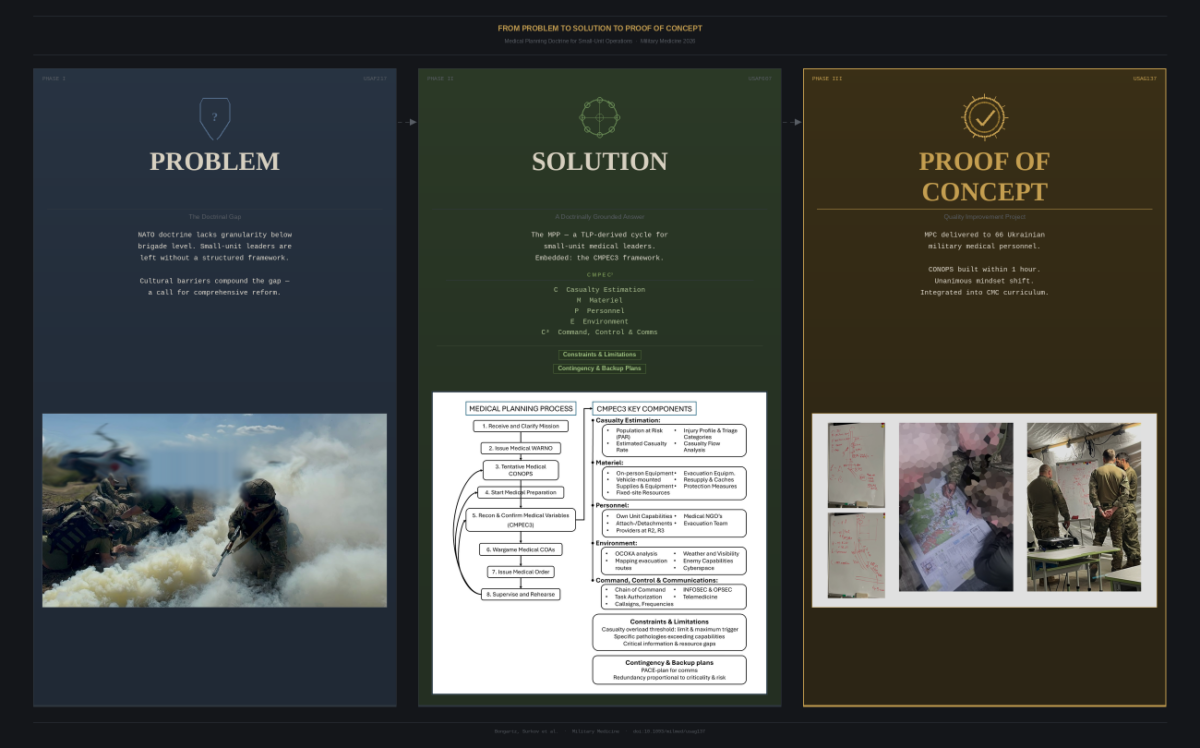
Casualty Estimation is the first and most foundational component of the CMPEC3 framework. Every subsequent planning decision — materiel quantities, personnel requirements, evacuation asset allocation, treatment facility positioning — flows directly from the casualty estimate. The MPP-CMPEC3 framework breaks Casualty Estimation into four sequential sub-components: Population at Risk (PAR), Estimated Casualty Rate, Casualty Injury Profile, and Casualty Flow Analysis.
Population at Risk
PAR defines the total number of people under the medical team’s responsibility within the area of interest. This is broader than it initially appears. It includes own forces, adjacent units, attached elements, civilian contractors operating within the area, wounded enemy combatants (per Geneva Convention obligations where applicable), service animals, and — in Ukraine’s operational context — the humanitarian volunteers and NGO personnel who frequently operate outside formal military governance structures. The involvement of medical NGO’s operating outside formal clinical and military governance, further complicates oversight and poses risks to operational security.
Accurately scoping the PAR prevents both under-planning (insufficient resources for actual demand) and over-planning (diverting scarce assets to groups not under medical responsibility). In a large-scale combat operation involving multiple SOF elements, conventional units, and host-nation forces, the PAR must be agreed and documented — not assumed.
Estimated Casualty Rate
Defining this number is an analytical act, not a concession of failure.
The MPP framework requires that the casualty estimate for units below Brigade level converges on a single agreed-upon number of casualties against which the medical plan is resourced.
This number should be informed by the tactical mission type — attack, defend, patrol, ambush — as well as the medical estimate derived from the MDMP, available trauma registry data, or operational experience. Where two or more COAs are under consideration in the Brigade planning process (e.g. most likely and most dangerous enemy COA), separate casualty estimates are developed for each, time allowing. The authors acknowledge that formulating a casualty estimate is challenging. A key question is at which echelon this estimate should be calculated. When absent or unreliable, we still advise doing a brisk but decisive casualty estimation to begin planning and to avoid “paralysis by analysis”.
Casualty Injury Profile
The Casualty Injury Profile characterizes likely wound patterns based on mission type, enemy capabilities, insertion method, and environmental factors. It involves selecting the probable ratio of Immediate, Delayed, Minimal, and Expectant triage categories.
For longer-duration missions, the profile should be divided per operational phase: for example Disease and Non-Battle Injuries (DNBI) during pre-staging, and battle casualties during execution.
Special considerations — hypothermia, chemical agents, altitude physiology, etc — are added based on mission-specific hazards.
The injury profile directly shapes materiel planning: a mission with a high proportion of penetrating trauma and blast injury requires different forward surgical and resuscitation capability than one dominated by DNBI and climate-related disease.
Casualty Flow Analysis
Casualty flow analysis estimates when and where casualties are likely to occur across the operational timeline and area of operations. This drives Casualty Collection Point (CCP) placement, evacuation route selection, and the distribution of medical assets across the battlespace. As the authors observe, “assume casualties can occur during any phase of the operation and determine efficient treatment locations and evacuation routes when constructing the evacuation scheme.”
This analysis is the direct precursor to the medical map overlay — the tangible planning product that makes the casualty estimate spatially actionable.
Medical plans must also realistically account for the limit trigger and maximum trigger thresholds, that determine when for example casualty redistribution is initiated or mission feasibility should be reassessed, respectively. This will be addressed in the Constraints & Limitations section.
#MilitaryMedicine #CMPEC3 #CasualtyEstimation #MedicalPlanning #NATOMedical #SmallUnitForces #CombatMedicine #LSCO #ForwardMedicine #MedicalMissionAnalysis
 MISSION REPORT- MARCH/APRIL 2024
MISSION REPORT- MARCH/APRIL 2024